Hearing Aids for Seniors in India
DEB's Audiology & Hearing Care
By DEB’s Audiology Team – May 2026 – 12 min read
In India, an estimated 27,000 children are born with significant hearing loss every year — and a significant number are not identified until developmental delays have already begun. The BERA test (also called the ABR test) is the gold standard for diagnosing hearing loss in infants and children who cannot participate in standard behavioural hearing tests.
This article covers:
The key takeaway: A BERA referral is not a confirmation of hearing loss. It is the investigation that gives parents and clinicians a definitive, accurate answer — and a clear path forward.
If your baby has been referred for a BERA test, you are probably worried. That is entirely normal. Being told your newborn needs further hearing investigation is frightening for any parent.
This guide will explain what the BERA test is, why it has been recommended, what happens during the test, and what the results mean – in plain language, not medical jargon. The BERA test is safe, painless, and one of the most important diagnostic tools in paediatric audiology.
If you have been searching online, you may have encountered multiple names for this test: BERA, ABR, BAER, BAEP, and Auditory Brainstem Response. These are all the same test. The terminology varies by hospital, country, and medical tradition, but the procedure and the information it provides are identical.
In India, the term BERA (Brainstem Evoked Response Audiometry) is most commonly used by hospitals and paediatricians. Internationally, ABR (Auditory Brainstem Response) is the standard term. Throughout this article, we use BERA because that is the term you are most likely to have heard from your doctor – but if you see ABR elsewhere, know that it is the same investigation.
Important distinction: BERA (the diagnostic test described in this article) is not the same as AABR (Automated ABR). AABR is the automated, bedside screening version used in hospitals in the first days of life – it gives a quick pass or refer result. BERA is the full diagnostic follow-up, performed in an audiology clinic, that provides detailed threshold information about your child’s hearing.
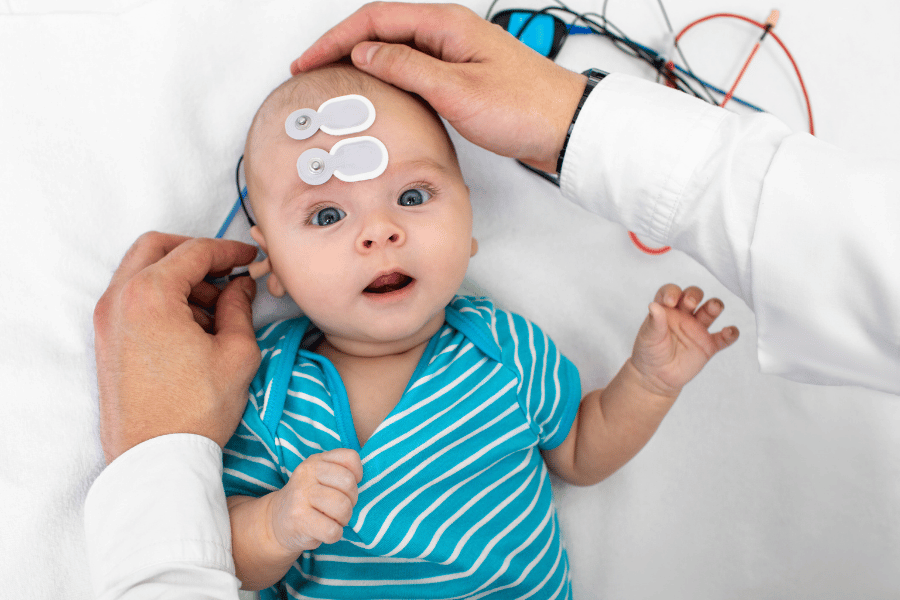
The BERA test measures how sound travels from your child’s ear through the auditory nerve to the brainstem. It does this by playing a series of clicking sounds through small earphones and recording the brain’s electrical response using sensors placed on the head.
The test produces a series of waveforms (labelled Wave I through Wave V) that show how the auditory signal is processed at each stage of the pathway. The audiologist analyses the timing, shape, and amplitude of these waves to determine two things:
Critically, the BERA test does not require the child to respond, cooperate, or be awake. The brain’s response is recorded automatically. This is why it is the gold standard for hearing assessment in infants and young children who cannot participate in standard hearing tests.
The most common reason for a BERA test is a failed or inconclusive newborn hearing screen. But it is also used in several other clinical situations:
This is one of the most common questions parents ask, and the distinction matters:
OAE (Otoacoustic Emissions) is a screening test that checks whether the cochlea (inner ear) is producing sounds in response to stimulation. It is quick, automated, and typically the first test a newborn receives. OAE tells us whether the cochlea is functioning – but it cannot assess the auditory nerve or the brainstem pathways beyond the cochlea.
BERA is a diagnostic test that examines the entire auditory pathway – from the cochlea, through the auditory nerve, to the brainstem. It provides detailed threshold information and can identify where in the pathway a problem lies.
OAE screens the cochlea. BERA confirms or rules out hearing loss and identifies where in the pathway any problem lies. A “refer” on the OAE is the start of the diagnostic process, not the conclusion
Before the Appointment:
For infants under three months, natural sleep during the test is usually achievable. You can help by keeping your baby awake in the car on the way to the appointment, feeding them just before the test begins, and bringing comfort items – a favourite blanket, a dummy, a familiar muslin.
For older infants and toddlers who are less likely to sleep naturally, mild sedation may be recommended. If this applies to your child, your audiologist will advise you in advance about fasting requirements and what to expect. Sedation for BERA is very mild – a small oral dose – and the child wakes normally within an hour or two.
Wash your baby’s hair with a gentle shampoo before the appointment and avoid applying oils or lotions to the head or face. Clean skin ensures good electrode contact. Dress your baby in comfortable clothing that allows easy access to the forehead and behind the ears.
During the Test:
Once your baby is settled or asleep, the audiologist will clean three small areas of skin – the forehead, the mastoid (the bony area behind each ear), and the top of the head – using a mildly abrasive gel. This improves electrical contact and takes about two minutes. Small, soft electrode patches are then applied to these areas. No needles are used at any point.
Foam insert earphones or small ear tips are placed in the baby’s ears. The test equipment plays a series of clicking sounds at different volumes and frequencies. The electrodes record the brain’s response to each sound automatically.
The most important thing during this phase is that your baby stays still. Movement creates electrical interference that affects the recordings. A sleeping baby produces the cleanest results. If your baby stirs, the audiologist will pause and allow them to settle before continuing.
You can stay in the room throughout the entire test. The test itself takes approximately 45–90 minutes depending on how settled the baby is and how many frequencies need to be tested.
After the Test:
The electrodes are gently removed. There is no recovery time – your baby can be fed, held, and taken home immediately. If mild sedation was used, the audiologist will monitor your child until they are fully awake, which typically takes 1–2 hours.
Your audiologist will explain the results to you on the same day in most cases. If the results require additional analysis or consultation, you will be informed of the timeline.
BERA results are presented as waveforms on a graph. Your audiologist interprets these, but here is what you should understand:
Your audiologist will explain exactly what the results mean for your child and what the recommended next steps are. No parent should leave a BERA appointment without a clear understanding of the outcome and the plan.
If the BERA confirms hearing loss, the next steps depend on the type and degree of loss identified:
A failed BERA test is not the end of a conversation – it is the beginning of an intervention plan. Early diagnosis and early action lead to significantly better outcomes for speech, language, and cognitive development.
At DEB’s Audiology, we work with families from diagnosis through intervention, including hearing aid fitting, therapy coordination, and ongoing monitoring.
At DEB’s Audiology, we provide a calm, child-friendly environment, same-day results in most cases, and clear guidance on next steps. Book your appointment.
Call or WhatsApp:
+91 88507 69404
Email: info@debsaudiology.com
Click to Chat